

Essential Tremor: The Mysterious Ailment and How Yoga Might Help
by Anthony Connell, E-RYT 500, CYS
Imagine having a disease with no known cause. This is what a diagnosis of “Essential Tremor” (ET) is for patients. ET is the most common cause of tremors, as well as one of the most common neurological conditions. A most basic definition of tremor is the involuntary and most times rhythmic shaking of any part of the body. Because of this, ET is often confused with Parkinson’s Disease. Although these two diseases are very similarly related, and ET can sometimes lead to Parkinson’s, they are entirely different diagnoses. Other notable neurological diseases include Multiple Sclerosis and Lou Gehrig’s disease (ALS).
What is Essential Tremor?
Essential Tremor, like Parkinson’s, is the involuntary movement of the head, neck, extremities, trunk, or any combination of the aforementioned, but the hands are especially affected. Unlike other forms of involuntary movement, scientists and doctors have not pinpointed a exact cause for ET, and thusly, it has become a diagnosis when no physical underlying abnormality can be readily seen through testing. One of the pitfalls of ET is that it can really only be studied through cadaver brain cells, which can be difficult to obtain. In fact, essential tremor really was not rigorously studied until Columbia University established the Essential Tremor Centralized Brain Repository in 2003, where brain tissue from ET donors is collected, processed and compared to age-matched brains that do not have ET. Even though there is a shortage of donor brains to be tested, the Repository has found that in fact there are subtle changes in the brain tissue of people who have tremor disorders, as will be discussed later. Firstly, let’s discuss the brain, as well as what a nerve cell is and its many functions.
Brain and Neuron Anatomy

The brain is the most complex organ in a vertebrates body, and is also the center of the nervous system, with its primary function being to exert centralized control over the other organs of the body, as well as deal directly with information processing, perception, motor control, arousal, homeostasis, motivation, pain, learning and memory. It is located in the head, near the primary sensory organs for vision, hearing, balance, taste, and smell. The brain also is considered to be where the “mind” is located, but obviously there is no proof of this. The nervous system, with the brain at it’s center, is comprised of tissue and nerve cells, called neurons, that extend thru-ought the body. The cerebral cortex, for example, which is the largest part of the brain, contains an estimated fifteen to thirty-three billion neurons alone. Neurons form intricate networks separated only by tiny gaps, called synapses. Neurons and the associated synapses are specialized for bodily communication. This occurs because neurons are electrically excitable cells, which allows them to transmit information to all parts of the body. The brain not only communicates in this fashion; in fact, it can also communicate through hormones.
In yoga therapy, one of the most noticeable abnormalities of brain function would be through motor control, whereby muscle movement is impaired in some way. Motor control falls under two different categories: voluntary and involuntary, where reflexes fall under the latter category.
A special characteristic of neurons, and what often makes healing a very arduous and sometimes impossible task, is that these cells do not replicate easily. The only way neurons are replaced is when stem cells, which are stored in the body, are converted into neurons in a process called neurogenesis. That being said, the only areas of the brain where neurons do seem to regenerate and go through cell division with consistency, and this has been discovered in recent years, is in the hippocampus and the olfactory bulb. There are many conflicting studies about a neuron’s ability to regenerate or be replaced, but one can say that although the brain is changing thru-ought our lifetime, these cells are meant to last. Many external factors, as well as disorders and diseases can often cause these cells to die prematurely, including drug use, stress, alzheimer’s disease, ingestion of aspartame, and sleep deprivation.
So what exactly is the anatomy of a nerve cell, and how can a neuron disrupt normal motor control? A neuron, unlike other cells in the body, have receiving branches (called dendrites), a main body (called the soma), nerve fibers (called axons) that conduct impulses away from the soma, and extremities (called terminal buttons) in which electrical impulses are transmitted from one cell to another. Although awkward looking at first glance, their shape is extremely important for carrying out their job inside the body. The signal is received by a cell through the dendrites by neurotransmitters (chemicals), and then travel down the cell as an electrical impulse to the terminal buttons, where more neurotransmitters are released to the next neurons. The axons, or the tail end of the cell actually can end with direct contact with muscles, and some axons are as long as one meter! The axons are covered in a fatty membrane called the myelin sheath which help conduct electricity, and this, is where many scientists believe tremors originate.
Research Findings
Columbia University’s Essential Tremor Repository did numerous studies on ET, and has found some promising findings that show more of where and why ET occurs. As stated earlier, ET was originally so mysterious that scientists did not even know what caused it to occur, and in fact, could not find any differences between healthy patients without ET and patients affected with ET. This is now not the case. Findings have showed that there are possibly two different subtypes of ET, which occur in different parts of the brain.
Subtype one is associated with the cerebellum, which is the part of the brain that handles movement and coordination. Inside the cerebellum are the largest type of neuron called a Purkinje cell, named after the man who discovered them. Three out of four cases of ET seem to be related to this subtype of tremor, where there is a loss of, or change to Purkinje cells. The change is found within the axon of the cell, where an abnormal swelling (torpedo) occurs, which then disrupts normal functioning. This subtype is related to a younger onset of the disease, as well as a familial history of Essential Tremor. Thusly, it seems to be related with genes.
The second subtype is related to another area of the brain called the locus coeruleus. The locus coeruleus is located in the upper brain stem and is associated with the physiological responses to stress and panic. This subtype accounts for the remaining quarter of patients with ET, and is closely related to changes found in patients with Parkinson’s disease. With this subtype, Lewy bodies, which are abnormal accumulations of substances (usually proteins), gather inside the nerve cells and disrupt normal function. As more Lewy bodies accumulate, the more disruption in brain function occurs.
Although these findings do not bring a cure to the table, they have brought scientists one step closer to finding out more about tremor disorders, as well as finding more specialized medications that can target these specific locations of the brain and its chemistry.
History and Presentation
Written records about tremors have been around for thousands of years, coming from places such as Egypt, Israel, and Greece. There are two main types of tremors: action tremors and at-rest tremors. Essential tremors hallmark feature are action tremors, while Parkinson’s, for example, are seen during both action and at-rest. An action tremor is simply a tremor that occurs during voluntary movement, whereas an at-rest tremor occurs while the muscle is not being stressed in any way. Most cases of ET occur later on in life, usually in the 60’s or older, but there are cases that occur at much younger ages. The most frequent clinical symptom reported and observed is action tremor. The tremor occurs when the hands are being used actively to perform voluntary activities such as writing, pouring, eating, and other daily activities. Patients with severe ET also have postural tremor, which appears when the arms are held outstretched in front of the body. Tremors in ET most commonly affect the arms, but they may also affect the head, voice, and occasionally the trunk and lower extremities. ET also can affect memory and the ability to translate thoughts and ideas into muscle movement. Some recent studies have shown postural instability and ataxia (irregular body movements due to defective muscular control), and cognitive abnormalities, specifically, problems with verbal fluency and memory to also affect patients with ET. To be clear about the difference between ataxia and tremors; ataxia is a diagnosable neurological dysfunction related to muscular coordination and tremors are involuntary movement associated with normal muscular control, whether at rest or in action.
Even though in the past ET was labeled "benign," scientists now know that the tremors are usually progressive, producing disabilities with basic daily life activities such as eating, writing, reading, personal care and driving. Severely affected end-stage patients are physically unable to feed or dress themselves. In these, the tremor can prevent any normal activities, which could result in a substantial loss of independence and even incapacitation in some cases. There is no way of knowing how quickly a patient will deteriorate, but the average patient has low to moderate deterioration.
Case Study
Andrew Samuel Connell was born in 1948 in the city of Trenton, New Jersey. He grew up in a poor to middle income household with his mother and his brother. They moved to Florida when he was approximately 8 years old. He is of Italian-Irish descent. His tremors are moderate, and especially noticeable when he tries to bring a glass to his mouth to drink. He has had tremors for as long as he can remember, and he has, through many years of dealing with them, learned to adapt to them so that he has not been affected by them too negatively. One thing I did notice was that he, many times, underplayed the severity of his tremors and his reaction to them, almost as though saying they bothered him were to show weakness in some way.
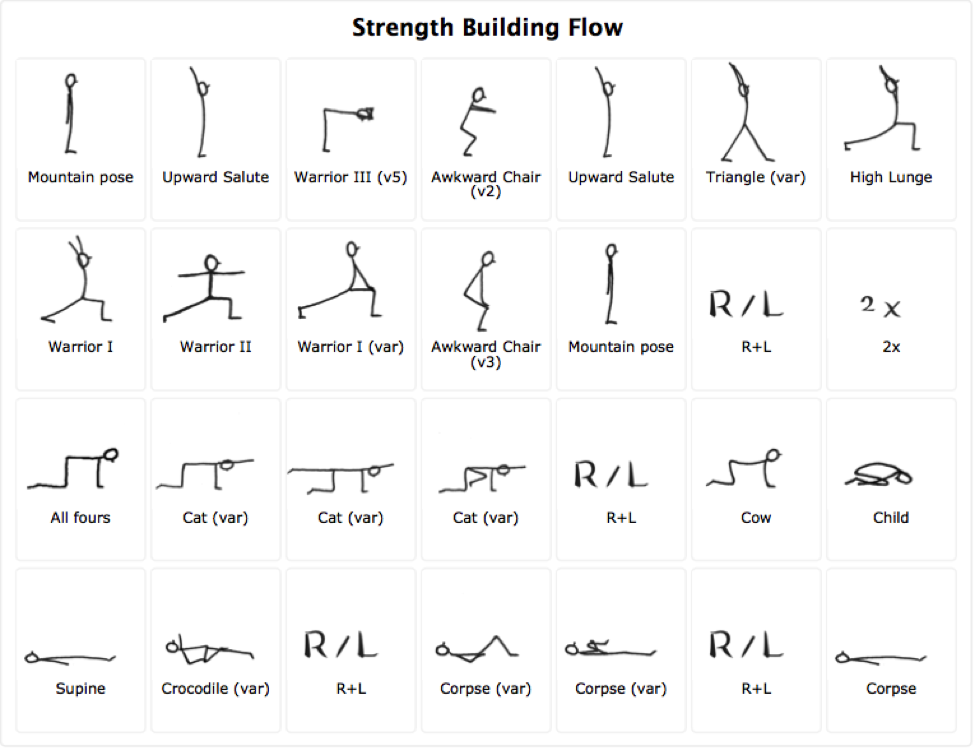
When we started, we had to be very careful since he is a cardiac patient with coronary artery disease. Initially, the primarily goal was to get him comfortable with doing yoga, since he was always second guessing whether he should or shouldn’t be doing the poses. I decided to alternate between a slow, gentle flow with longer held postures for stability and to try and allow him to sink into his own form of meditation and a more muscle strengthening flow, albeit both were slow in nature. For the strengthening flow we always used a chair that was around waist height, in order to keep him aware of not bringing his head below his heart.
We met three times a week twice a month, with each week being dedicated to one specific flow. For homework he was to a shortened version of the gentle approach since I wanted to make sure that, while unsupervised, he was doing non-vigorous postures and nothing that would potentially cause any cardiac events. After only a month, he could tell that the tremors were not as noticeable, however, stress or anxiety would flare them up. This was something we worked on extensively at that point, giving him the tools to use calming techniques outside of class in order to try and keep his stress levels down. Listed below are both sets of flows.
During Savasana, I would give him time either in silence or with a bit of soft music in order to help him process the practice, and then, on occasion, do a guided meditation. Along with the actual asana practice, we usually did a lot of pranayama, including a more gentle Khapalabati, Sitali, as well as Alternate-Nostril breathing. A small change we made was to have him cut back on caffeinated tea, specifically his favorite and only tea he drinks, Earl Grey. We cut it back to only two to three cups a day, and never at night, which he would do. In fact, he would drink it constantly all day long on his days off from work. We tried herbal teas, but he has a specific pallet and hasn’t warmed up to the idea of any other type of tea.
He has said that he plans on continuing his practice even though I won’t be guiding him as much because he felt like it did help, which in my belief, is where I ultimately wanted him to be. As long as he feels like he has the ability to alleviate symptoms associated with his tremors, he can achieve anything he sets his mind to.
References
Essential Tremor Centralized Brain Repository
International Essential Tremor Foundation
"A Neuroscience Field Guide: The Purkinje Cell"
Yoga Wiz: Exercises for Tremors

Anthony Connell, E-RYT 500, CYS, is a graduate of Florida International University with a degree in psychology and is presently a Clinical Yoga Therapy candidate at AUM hOMe Shala. Tony teaches for AUM's annual Chill Out program in inner-city schools, and also teaches yoga in after-school programs and assists with AUM’s 200-Hour Yoga Teacher Training. Tony began his practice in 2002 and loves to share the benefits of yoga for maintaining balance and alleviating stress.